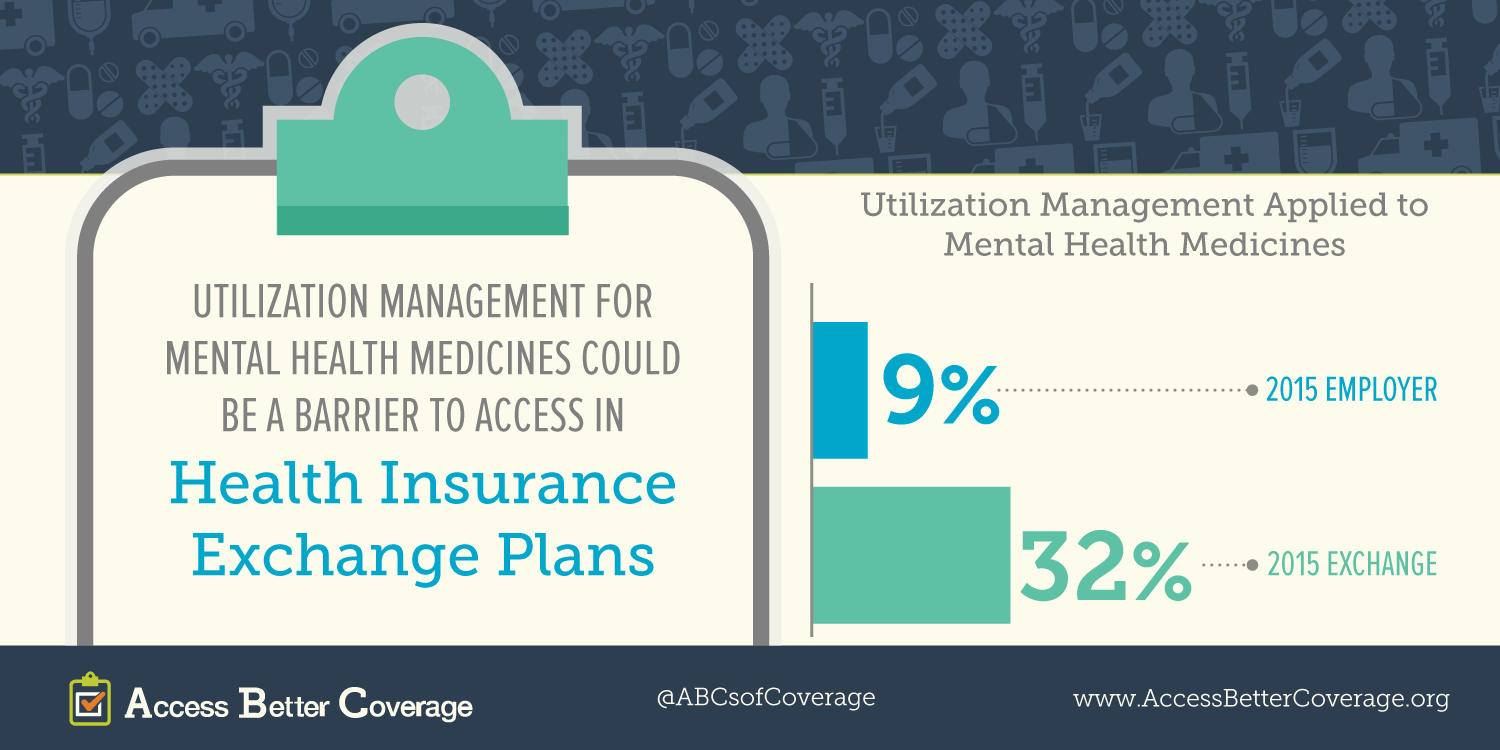
Patients, especially those suffering from chronic conditions, deserve access to the medicines they need to live longer, healthier lives. Today, PhRMA released a new fact sheet on access to mental health medicines in exchange plans in 2015 (2014 fact sheet is available here). The fact sheet highlights some of the potential barriers to accessing needed treatments. Learn more on AccessBetterCoverage.org, in our patient profiles and our other fact sheets.
This is the first in our Q&A series with patient advocates. We talked with Andrew Sperling, director of federal legislative advocacy for the National Alliance on Mental Illness (NAMI).
Question (Allyson Funk, PhRMA): What is NAMI and who do you represent?
Answer (Andrew Sperling, NAMI): NAMI is the largest organization representing and advocating on behalf of people living with severe mental illness and their families. We have 1,000 state and local organizations involved in advocacy, education and research on serious mental illness, defined as a limited number of severe disorders including schizophrenia, bipolar disorder, major depression, seasonal affective disorder, and anxiety disorders including post-traumatic stress disorder (PTSD).

NAMI is in all 50 states and run by volunteers, including people living with serious mental illness and their families. Because of onset of disorders in late adolescence and early adulthood, families are really the bedrock of our organization.
Q: How do medicines help patients manage mental health conditions?
A: Medicines are the backbone of treatment interventions available today. They are not perfect, but they are very effective at helping people function at a higher level. They are not disease modifying agents or cures, but we do have more effective treatments. We need innovation on two levels:
- Searching for disease modifying therapies.
- Incremental improvements to address some of the negative and disabling side effects of these conditions, including social withdrawal and cognitive impairment, which can make a huge improvement in the lives of people living with these conditions.
Q: The Affordable Care Act (ACA) expanded health insurance coverage to a broader population. What are you hearing about coverage in health insurance exchanges, in particular access to mental health medications?
A: There is good news and bad news. The ACA has been enormously important in improving and expanding coverage for patients with severe mental illness, particularly in states who expanded Medicaid eligibility.
The challenge we face is with the level of coverage that some people are getting with exchange plans. While it’s important for them to move from the ranks of the uninsured and have that stability of health insurance coverage, we have seen a number of states where there are barriers to getting meaningful coverage for the medicines their physicians prescribe.
We’ve seen a significant amount of aggressive utilization management, particularly for classes like anti-psychotics. We see placement of medicines on the highest (4th and 5th) tier where medicines face not a copay but coinsurance. High cost sharing can often serve as a significant barrier and we’re very concerned with that.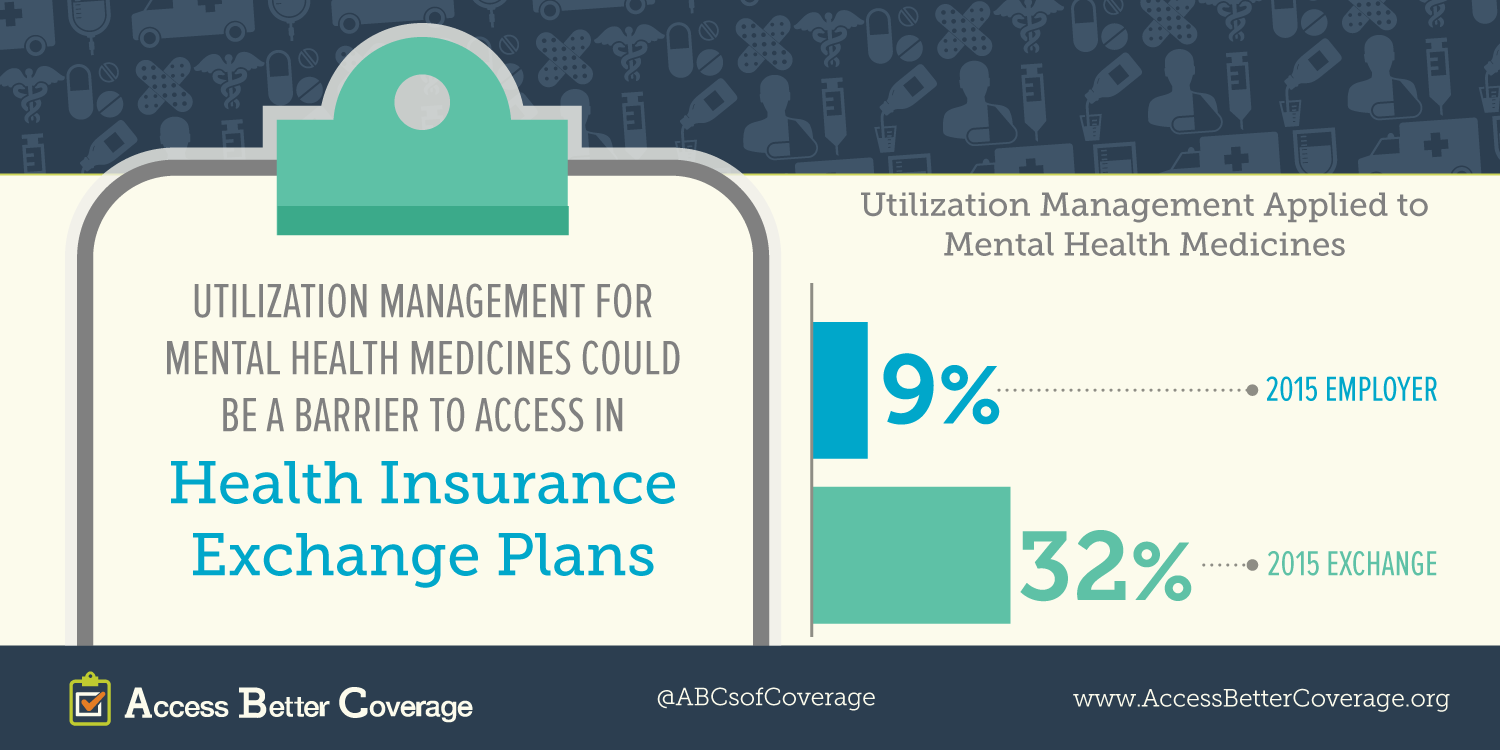
We’ve also seen aggressive use of step therapy and fail first: where an individual patient has to fail first on a particular compound before getting access to the one their doctor prescribed. This is troubling because treatment failure can be complicated for someone living with mental illness; it’s often defined as because of psychosis or mania or severe depression. That’s concerning because treatment failure can be very complicated for someone living with mental health disorders. Even when a patient rebounds they may never get back to where they were before. We have real concerns about high use of step therapy and prior authorization in these exchange plans.
Q: What are the biggest concerns facing mental health patients in health exchanges?
A: Utilization management and the proliferation of policies like fail first and step therapy: we’re hearing the most complaints about use of step therapy and prior authorization.
Q: Is there anything else we missed?
A: We did a study [“A Long Road Ahead: Achieving True Parity in Mental Health and Substance Abuse Care”] to examine some of these policies in the largest exchange plans. We also wanted to look at how exchange plans are meeting obligations to comply with the Mental Health Parity and Addiction Equity Act. But we need more data to ensure plans are complying with that law, which requires plans to cover treatment for mental illness under the same terms and conditions as medical and surgical disorders. There is some indication there is compliance with the numerical or quantitative side of parity, but there is some evidence that there isn’t widespread compliance with the qualitative side of parity. This is concerning in the area of prescription drugs because we want to make sure plans are not imposing things such as step therapy and prior authorization disproportionately on medicines to treat mental illness.