Is 340B benefiting the vulnerable, uninsured patients it was designed to help? Evidence continues to show otherwise. An updated analysis from Berkeley Research Group (BRG) is the latest to build on other studies, finding the program may actually be raising patient costs by driving care from physician offices to the more expensive hospital outpatient setting.
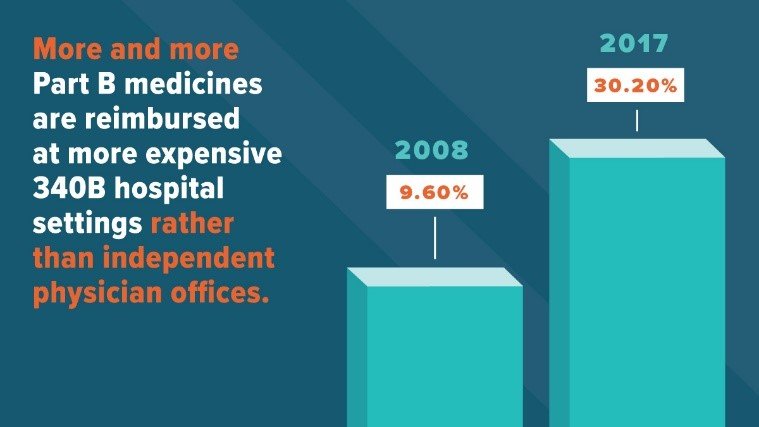
Looking at all Medicare Part B reimbursement for physician-administered medicines, BRG found that more than 30 percent of reimbursements were at 340B hospital settings in 2017. That’s up from less than 10 percent in 2008.
The report also found that the share of reimbursement at 340B hospitals for breast cancer, rheumatoid arthritis and multiple myeloma treatments continued to increase from 2016 to 2017 while decreasing in the physician practice setting. In fact, more than 38 percent of breast cancer and multiple myeloma treatments and more than 21 percent of rheumatoid arthritis treatments were at 340B hospitals in 2017. This is a continued increase from the last report looking at the increase from 2008 to 2015.
The 340B program incentivizes participating hospitals to purchase independent physician offices to expand the reach of the 340B program and bring in more profit by registering these entities as their offsite outpatient sites. This consolidation is at the expense of patients. For example, patients with commercial insurance end up paying more out of pocket in the form of cost sharing and premiums for medicines administered at hospital settings than they do at independent physician offices. And studies have noted that 340B “will ultimately end up increasing health care costs for everyone” as a result of this shift in site of care.
As evidence continues to mount, policymakers must not ignore these warning signs and need to instead continue to push for legislation to improve the 340B program and ensure it benefits patients, not large hospitals.
To learn more about the 340B program and ways it could be fixed, visit PhRMA.org/340B.


