 Recent studies show the Affordable Care Act (ACA) has reduced the uninsured rate and lowered the amount of uncompensated care that hospitals provide. Paradoxically, these welcome trends are also contributing to growth in the 340B program. The program was created in 1992 to assist health care providers receiving federal grants and true safety net hospitals – those serving large numbers of uninsured or vulnerable patients – by making them eligible for deeply discounted pharmaceuticals to increase patient access to medicines. It is important for the program to continue, which is why concerns have recently been raised[i] about the long term sustainability of the program in light of the explosive program growth in the age of the ACA. Specifically, current 340B program eligibility criteria used for hospitals means more hospitals are qualifying for the program just as hospitals are benefiting from declines in the number of uninsured and uncompensated care.
Recent studies show the Affordable Care Act (ACA) has reduced the uninsured rate and lowered the amount of uncompensated care that hospitals provide. Paradoxically, these welcome trends are also contributing to growth in the 340B program. The program was created in 1992 to assist health care providers receiving federal grants and true safety net hospitals – those serving large numbers of uninsured or vulnerable patients – by making them eligible for deeply discounted pharmaceuticals to increase patient access to medicines. It is important for the program to continue, which is why concerns have recently been raised[i] about the long term sustainability of the program in light of the explosive program growth in the age of the ACA. Specifically, current 340B program eligibility criteria used for hospitals means more hospitals are qualifying for the program just as hospitals are benefiting from declines in the number of uninsured and uncompensated care.
According to a January analysis by Gallup, the uninsured rate has dropped by 4.2 percentage points since the ACA went into effect in January 2014.[ii] Not surprisingly, this has resulted in hospitals seeing more insured patients with access to affordable medicines. Last week the Department of Health and Human Services (HHS) released a report[iii] showing hospitals provided an estimated $7.4 billion less in uncompensated care in 2014 as a result of ACA coverage.
 What does this decrease in uncompensated care mean for hospitals’ bottom lines? Some hospitals that had made large projections for 2014 revenue increases based on the ACA saw their revenues increases as much as double over initial projections in the first year of Medicaid expansion and Health Insurance Exchange operation.[iv] This added revenue likely comes from the steep drop in uncompensated care reported by HHS. In states that expanded Medicaid, hospital uncompensated care declined by 26 percent. In non-expansion states, uncompensated care declined 16 percent.[v]
What does this decrease in uncompensated care mean for hospitals’ bottom lines? Some hospitals that had made large projections for 2014 revenue increases based on the ACA saw their revenues increases as much as double over initial projections in the first year of Medicaid expansion and Health Insurance Exchange operation.[iv] This added revenue likely comes from the steep drop in uncompensated care reported by HHS. In states that expanded Medicaid, hospital uncompensated care declined by 26 percent. In non-expansion states, uncompensated care declined 16 percent.[v]
Why is a decline in hospital uncompensated care associated with more facilities qualifying for a program designed to help true safety net facilities? The answer lies in how many hospitals qualify for the 340B program. The vast majority (81 percent) of all 340B sales volume originates from hospitals that qualify for 340B on the basis of their disproportionate share hospital (DSH) percentage.[vi] This percentage is a measure based on the number of Medicaid and low-income Medicare patients treated on an inpatient basis. The DSH formula does not account for the share of uninsured patients a hospital sees. This means if a hospital has many patients transitioning from being uninsured to having Medicaid, that hospital would become more likely to qualify for 340B just as its burden of caring for the uninsured was declining.
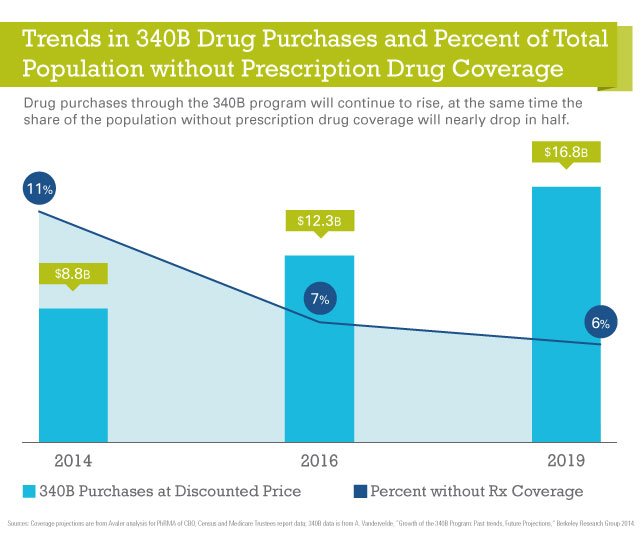
A 2014 study by the Berkeley Research Group[vii] found the 340B program has already seen total sales at the 340B price increase from $1.1 billion in 1997 to more than $7 billion by 2013, and there are no signs growth is slowing. By 2019, it is estimated total sales at the 340B discounted price will reach $16.8 billion—90 percent more than the $8.8 billion in 340B volume in 2014.[viii]
 The original intent of the 340B program was to reduce outpatient drug costs for uninsured or vulnerable patients. Since the program’s inception, developments within the program that could not have been anticipated by the law’s drafters have combined with a lack of sufficient guidance from HHS to create a perfect storm leading to uncontrolled and unsustainable growth in the program.
The original intent of the 340B program was to reduce outpatient drug costs for uninsured or vulnerable patients. Since the program’s inception, developments within the program that could not have been anticipated by the law’s drafters have combined with a lack of sufficient guidance from HHS to create a perfect storm leading to uncontrolled and unsustainable growth in the program.
Future growth will in part be fueled by a Medicaid expansion that is strengthening hospitals, raising serious questions about using the DSH metric to determine hospital eligibility for the 340B program. With the number of insured Americans on the rise, and the amount of uncompensated care provided by hospitals decreasing by billions of dollars, now is the time to revisit how hospitals qualify for 340B to ensure that the program is sustained so that it can serve the entities that truly serve uninsured or vulnerable populations both today, and for future generations to come.
[i] House Energy and Commerce Committee, Subcommittee on Health on "Examining the 340B Drug Pricing Program" March 24, 2015.
[ii] Levy, Jenna. “In U.S., Uninsured Rate Sinks to 12.9%,” Gallup. January 2015. (Available at: http://www.gallup.com/poll/180425/uninsured-rate-sinks.aspx)
[iii] Office of the Assistant Secretary for Planning and Evaluation. “Insurance Expansion, Hospital Uncompensated Care, and the Affordable Care Act,” HHS. March 2015. (Available at: http://aspe.hhs.gov/health/reports/2015/MedicaidExpansion/ib_UncompensatedCare.pdf)
[iv] Galewitz, Phil. “Safety Net Hospitals Already Benefit from ACA,” Kaiser Health News. May 2014. http://www.medpagetoday.com/Washington-Watch/Reform/46035
[v] Office of the Assistant Secretary for Planning and Evaluation. “Insurance Expansion, Hospital Uncompensated Care, and the Affordable Care Act,” HHS. March 2015. (Available at: http://aspe.hhs.gov/health/reports/2015/MedicaidExpansion/ib_UncompensatedCare.pdf)
[vi] Sales data from Apexus Update 2015 – 340B Coalition Winter Meeting;
[vii] Vandervelde, Aaron. “Growth of the 340B Program: Past Trends, Future Projections.” Berkeley Research Group. November 2014. (Available at: http://www.thinkbrg.com/media/publication/524_Vandervelde_340B_GrowthDrivers_WhitePaper_20141202_FINAL.pdf)
[viii] Ibid.
Get updates on this subject and/or other relevant issues here. {{cta('4fe14269-44de-493b-a19c-946e0454614a')}}


