
How can a program originally designed to help the deserving clinics treating our nation’s most vulnerable patients be used instead to pad the bottom line of large hospitals often providing minimal charity care?
This is a question policymakers may be asking after seeing new data from the Berkeley Research Group on an obscure program called 340B.
Congress created the 340B drug discount program in 1992 to assist health care providers receiving federal grants and true safety net hospitals serving large numbers of uninsured and vulnerable patients by making them eligible for deeply discounted pharmaceuticals.
The program has seen explosive growth since its inception. And in recent years much of that growth has been driven by a change in policy allowing discounts to be shared with outside “contract” pharmacies.
The original intent of these pharmacy arrangements was to help small clinics without their own in-house pharmacy.
Instead all 340B entities – including large non-profit hospitals – are now allowed to have an unlimited number of contract pharmacies.
New data shows that large hospitals are aggressively using contract pharmacies. A new Berkeley Research Group analysis for PhRMA finds of the largest 20 percent of 340B hospitals (as measured by total outpatient revenue), 68 percent have at least one contract pharmacy. Of those with a contract pharmacy, 64 percent have more than 20 contract pharmacies. Past research has shown that large hospital contract pharmacy networks are not predominantly located in low-income areas and many are in relatively wealthy areas. [1]
By contrast, the safety-net clinics (known as HRSA grantees) that qualify for 340B discounts are much less likely to benefit from the contract pharmacy program. Fewer than one in five (19 percent) grantees have at least one contract pharmacy. Of grantees that have a contract pharmacy, 8.9 percent have more than 20 contract pharmacies.
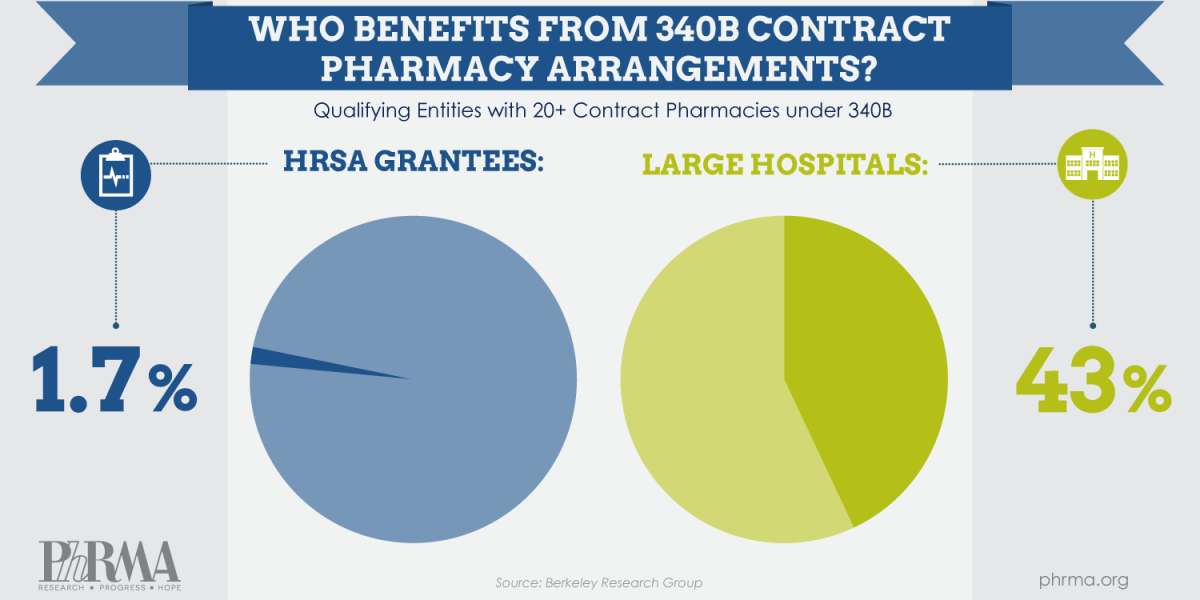
 That means less than 2 percent of all grantees have more than 20 contract pharmacies. In contrast, 43 percent of the largest 340B hospitals have more than 20 contract pharmacies. These clinics, by the nature of their federal grants, are required to reinvest revenue from 340B discounts into services for the vulnerable patients they serve. By contrast, hospitals in the 340B program face no requirements related to how revenue from 340B is used and are not required to report how they use money they gain through the program.
That means less than 2 percent of all grantees have more than 20 contract pharmacies. In contrast, 43 percent of the largest 340B hospitals have more than 20 contract pharmacies. These clinics, by the nature of their federal grants, are required to reinvest revenue from 340B discounts into services for the vulnerable patients they serve. By contrast, hospitals in the 340B program face no requirements related to how revenue from 340B is used and are not required to report how they use money they gain through the program.
This new data comparing hospitals and grantees use of contract pharmacy arrangements builds on questions that have been raised about the 340B program and contract pharmacies. A 2014 Department of Health and Human Services Office of Inspector General (OIG) report found of 15 disproportionate share hospitals (those qualifying for 340B) interviewed, more than half reported not offering the 340B-discounted price to uninsured patients in even one of their contract pharmacy arrangements, leaving these patients to pay the full non-340B price at the pharmacy counter. [2] Of the 340B entities included in the report that did offer the discounted price to patients, 72 percent were grantees. [3] Separate analysis from Avalere shows the majority of hospitals in the 340B program provide less charity care than the national average for all hospitals.[4]
This new data combined with the previous studies raises additional concerns regarding the contract pharmacy program and 340B program, which was created to help safety net providers that treat uninsured and vulnerable patients. This new data shows the entities most likely to benefit from contract pharmacies are less likely to pass along that benefit to needy patients, while the vast majority of the clinics dedicated to serving vulnerable populations get no benefit from the program.
View all 340B Spotlight Posts
Footnotes:
1] A. Vandervelde "Contract Pharmacy Mapping Analysis," Berkeley Research Group, June 2014 (Available at http://www.thinkbrg.com/publications-vandervelde-contract-pharmacy.html)
2] Department of Health and Human Services Office of Inspector General, "Memorandum Report: Contract Pharmacy Arrangements in the 340B Program," February 2014 (Available at: https://oig.hhs.gov/oei/reports/oei-05-13-00431.pdf)
3] All grantees included in the OIG study were Community Health Centers.
4] Alliance for Integrity and Reform of 340B, "Unfulfilled Expectations: An analysis of charity care provided by 340B hospitals," Spring 2014 (Available at: http://340breform.org/userfiles/Final%20AIR%20340B%20Charity%20Care%20Paper.pdf)


